
Why Erin Gray Felt More Lost with her Second Cancer
Even though patient navigation is proven to deliver better outcomes, few hospitals offer it.

The first time Erin Gray walked into her breast surgeon’s office to hear test results, the surgeon was already crying before she could say a word. Erin is a psychotherapist. She read it in under a second. She turned to her husband and said: I have cancer. He didn’t understand how she could possibly know yet. Erin had been watching faces for a living for fifteen years. The surgeon’s poker face was, in Erin’s words, the worst.
Full episode: Spotify | Apple | YouTube | Everywhere
What the surgeon said next mattered more than the diagnosis. Not the news. The choreography. Here is your oncologist. Here is when you’ll meet her. Here is the doctor who will do your hysterectomy. Here is your plastic surgeon. Here is the order of things. Erin had been carrying a BRCA2 mutation for over a year. She’d known this was coming. The surgeon didn’t hand her a packet. She handed her a map.
Eight years later, Erin sat in the same doctor’s office with a different diagnosis: papillary thyroid cancer. Not BRCA-related. Unrelated to the first. By every clinical measure, smaller. Less aggressive. Less surgery ahead. She should have been the most prepared patient on the schedule. She fell apart. The oncologist she’d known for years told her thyroid cancer wasn’t really “cancer-cancer,” shrugged, and walked out. The PA came back in and hugged her while she cried. Erin’s reaction surprised her: I didn’t have this with chemo. I didn’t have this with the mastectomy. Why now?
The Power of a Guide
The first time, Erin had a guide, and the second time, she didn’t. A guide is the person who, after the diagnosis, says these words: here is what happens next, and next, and next.
For Erin, the guide was her breast surgeon. When the second diagnosis fell outside that surgeon’s territory, the guide didn’t transfer. Erin had to assemble a team from scratch. The cancer wasn’t the destabilizing thing. Not having a map was.
What I’m describing might sound like emotional support. It isn’t. It’s a documented clinical intervention with thirty-five years of outcomes data.
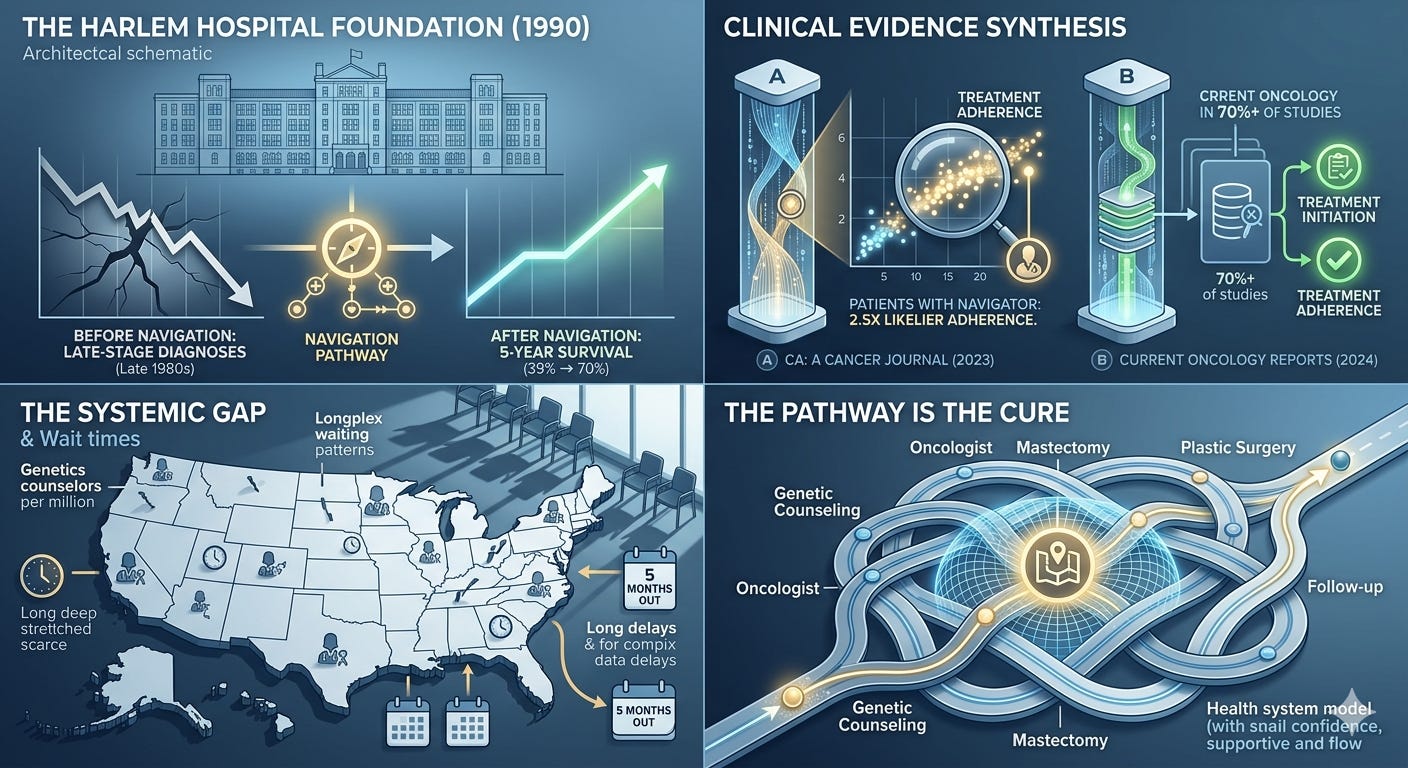
The Harlem Hospital Pilot (1990): The first patient navigation program in the United States started at Harlem Hospital in 1990, led by surgical oncologist Harold Freeman. His patients had been arriving with late-stage breast cancer at survival rates that were a national scandal. After he built a navigation program that walked patients from suspicious finding to resolution, five-year survival in that population went from 39% to 70%.
What the Data Shows
The intervening decades have produced more evidence than most oncologists know how to act on:
Study / SourceKey Finding
2023 Systematic Review
(CA: A Cancer Journal for Clinicians)
Patients with a navigator were two-and-a-half times more likely to adhere to treatment. (Source)
2024 Systematic Review
(Current Oncology Reports)
Navigation improved treatment initiation in 70% of studies and treatment adherence in 71%. (Source)
What Erin lost between cancer #1 and cancer #2 was not soft. It was the thing the data says moves outcomes.
A Systemic Gap
Erin had a guide the first time because her breast surgeon happened to be the kind of doctor who conducts. There is no system that requires it.
The American Cancer Society funded Freeman’s pilot in 1990, and there are still only about 2,500 certified genetic counselors in the entire United States (Source), roughly eight per million people. If you find out you carry BRCA1 or BRCA2 today, you are stepping into the same gap Erin stepped into before her first diagnosis.
Erika Stallings, whose mother had BRCA2 breast cancer, called for a genetic counseling appointment and was told the next opening was five months out. (Source)
That is not anomalous. That is the system working as designed.
I had a guide on my own genetic diagnosis without realizing how lucky I was. I was the third person in my immediate family to learn I was BRCA1 positive - and I had assumed it for years prior. My mother and sister were already on the map. The route was drawn in pencil before I was born. I had a geneticist talk with me before and after the DNA test and she share the map of my choices.
But when I was diagnosed with cancer, my hospital did not have (and still doesn’t have for breast cancer) a patient navigation team to guide me through the process. I was lucky because I’d been a caregiver so many times before that I knew the map. Most people don’t.
Finding Your Map
If you’re newly diagnosed, or carrying a known mutation, or supporting someone who is: who is your guide?
Not the doctor with the most letters after their name. The person who tells you the next three appointments, the next three weeks, the next three decisions. If your team has not named that person, name them yourself.
Ask the oncology nurse navigator at your hospital.
Ask the genetic counselor’s office.
Ask one of your doctors which person on the team to call first when you don’t know what to do.
The PA who hugged Erin in the exam room wasn’t supposed to be the guide for the second cancer. Nothing in the system told her to be. She just was. Sometimes guides appear. The rest of the time, you have to ask.
Matthew Zachary (episode 37) is leading a national movement for a Cancer Patient’s Bill of Rights that would include a patient navigator for EVERY person diagnosed in the US. It’s called WethePatients.org and worth a look.
Catch Erin’s complete episode of the podcast on your preferred platform: Watch on YouTube | Listen on Spotify | Listen on Apple Podcasts