
What the System Owes You And Why You Have to Fight to Get It
The survival gap: Why your recovery depends on who you know, not just what you have.

In January 2024, Medicare quietly did something that should have been front page news in every cancer center in America. For the first time, it established billing codes for principal illness navigation services — meaning a nurse navigator could finally be reimbursed for the time she spends helping a cancer patient get through treatment.
It took thirty-four years.
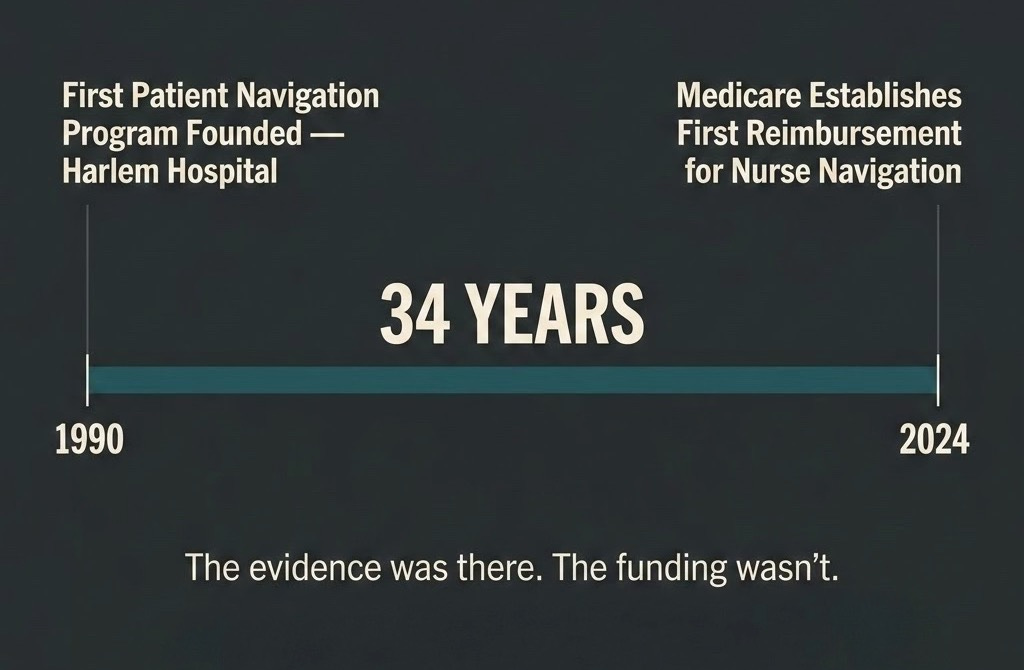
The first patient navigation program in the United States launched in 1990, created by Dr. Harold Freeman at Harlem Hospital, specifically to help underserved Black women access breast cancer care. The outcomes were immediate and measurable. Patients who receive navigation services have a shorter time to diagnosis and treatment, are more likely to complete their course of treatment, and report a better understanding of their condition, as well as an overall higher quality of life. Cancer Researchers have replicated those findings dozens of times since. And yet, for three decades, nurse navigators remained one of the most underfunded, inconsistently deployed, and frequently uncompensated roles in oncology.
That’s the backdrop for the conversation I had with Matthew Zachary.
Get the episode: Spotify | Apple | YouTube | Everywhere

Matthew was 21 in 1995 when he was diagnosed with medulloblastoma, a brain tumor typically found in young children. He got through surgery and radiation. Then his oncology team recommended prophylactic (preventative) chemotherapy. The protocol included two drugs that would cause permanent hearing loss and irreversible nerve damage in his fingers. Nobody mentioned that. His family found out because his uncle happened to be a geneticist and caught it before the first infusion. The information existed. It just wasn’t offered.
He refused the “preventative” drugs. His life was saved. But the experience left him with a question he has spent thirty years trying to answer: why does your outcome depend so heavily on what you happen to know, who you happen to know, and what you can afford?
What a Navigator Actually Does
When people hear “nurse navigator,” they sometimes picture someone who hands out pamphlets and schedules appointments. The research tells a different story.
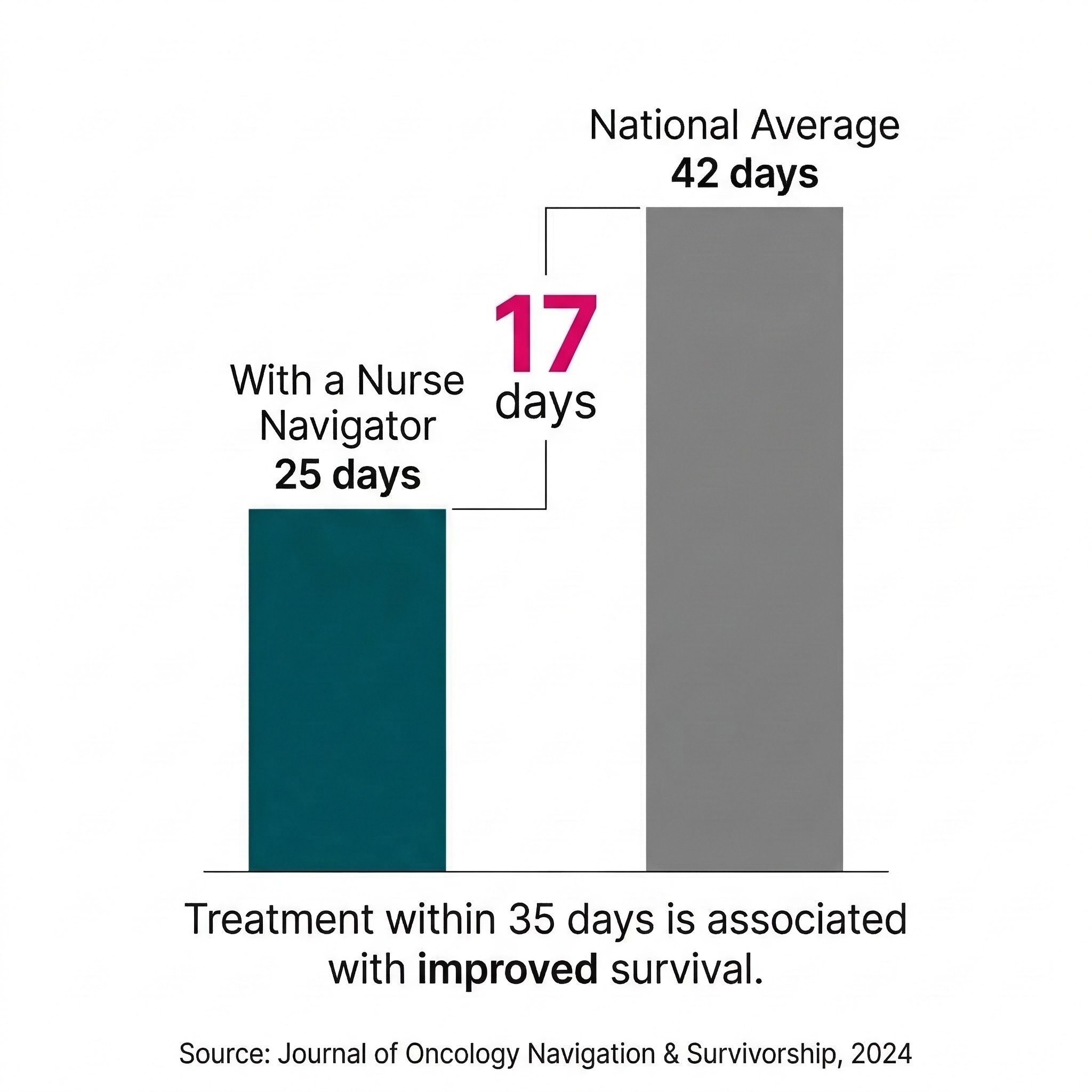
In a quality improvement study on lung cancer care, oncology nurse navigator involvement improved time from biopsy to initial consult by 18% — and the average time from biopsy to treatment initiation for navigated patients was 25 days, compared to the national benchmark of 42 days. Getting to treatment faster matters. A diagnosis-to-treatment interval of fewer than 35 days is associated with improved survival.
Underserved, rural, and economically disadvantaged patients with cancer who are under the care of an oncology nurse navigator are better prepared to begin treatment and require fewer services than non-navigated peers. Regular check-ins with a nurse have also been shown to improve breast cancer survivors’ quality of life, reduce fear of recurrence, and support mental health compared to standard physician follow-up.
The problem is access. Navigation services are often funded externally through grants or treated as unreimbursed administrative costs because, until January 2024, there was no reimbursement mechanism. Which means whether you got a navigator depended almost entirely on whether the hospital you happened to walk into had grant funding to pay for one.
That’s not a care system. That’s a lottery.
Get the episode: Spotify | Apple | YouTube | Everywhere
The Financial Side of This That Nobody Wants to Talk About
Matthew’s third protection — bankruptcy protections before treatment starts — is the one that most cancer organizations quietly sidestep. The data is hard to look at.
A 2024 Harvard Medical School study cited by US News & World Report, which was tracking nearly 100,000 cancer patients, found that survivors had five times higher odds of filing for bankruptcy compared to people without a cancer diagnosis. Their average credit scores were nearly 80 points lower — and the damage persisted for up to 9.5 years after diagnosis per ASCO. This was in Massachusetts, a state with mandated health coverage.
More than 40% of patients spend their entire life savings in the first two years of treatment. And that number doesn’t capture the full picture. Between 40% and 85% of cancer patients stop working during initial treatment, with absences ranging from 45 days to nearly six months. The mortgage doesn’t pause. The car payment doesn’t pause. The cost of getting to treatment — gas, parking, flights for those without a major cancer center nearby — doesn’t pause. Income stops. Everything else keeps going.
Cancer patients who declared bankruptcy had a nearly 80% greater mortality risk than those who did not, not because they had more advanced cancers, but because they had the same curable cancers, received the same treatments, and still died at higher rates.
Financial toxicity kills people. Not metaphorically. Measurably.
Matthew’s argument is that no patient should make decisions about whether to start, delay, or stop treatment based on what it will do to their credit score. Bankruptcy protections that activate before treatment begins — not after a patient has already lost everything — are the floor, not the ceiling.

Why the Voter Bloc Has Never Existed
Matthew is not subtle about this: the organizations that could have built a cancer patient voting bloc over the last thirty years didn’t, because their funding models depend on relationships with the same institutions that benefit from the status quo. Patient power was never the goal.
WeThePatients.org is built on a different premise. Fifty million Americans are affected by cancer. If even a fraction of them showed up to state legislatures with a unified ask — a reimbursable nurse navigator, a legally protected cancer steward, bankruptcy protection before treatment — the math changes.
He’s going state by state because that’s where health policy actually gets made, and because state legislators are more accessible than federal ones. He’s not waiting for the advocacy establishment to come around.
Get the episode: Spotify | Apple | YouTube | Everywhere
What You Can Do Right Now
Listen to the full episode. Then share it with someone who has been through cancer, is in it, or loves someone who is. Not as a gesture — but because this conversation gives people language for something they’ve been feeling and didn’t know how to name.
The system was built for people who already know how to navigate it. Matthew is trying to change that. You can be part of it at WeThePatients.org.
Links
President’s Cancer Panel — Patient Navigation Report https://prescancerpanel.cancer.gov/reports-meetings/enhancing-patient-navigation-2024/achieving-equity-cancer-care
Journal of Oncology Navigation & Survivorship — Lung Cancer Nurse Navigation Study (2024) https://jons-online.com/issues/2024/february-2024-vol-15-no-2/5031:incorporating-upstream-oncology-nurse-navigation-to-improve-timeliness-to-treatment-in-lung-cancer-a-quality-improvement-project
HealthDay / U.S. News — Harvard/Beth Israel 2024 Bankruptcy Study https://www.usnews.com/news/health-news/articles/2024-10-18/a-cancer-diagnosis-takes-devastating-toll-on-family-finances
STAT News — Financial Toxicity and Cancer Costs https://www.statnews.com/2023/05/23/financial-toxicity-cancer-costs-cost-sharing/
PMC — Washington State Cancer Bankruptcy Study https://pmc.ncbi.nlm.nih.gov/articles/PMC4240626/