
The Mountain Her Doctor Was Afraid Of
How a cancer survivor traded the sofa for a trailhead, and the hidden data that proves she was right to do it.

The elevator in the Vegas hotel was the glass kind, the kind that lets you watch the lobby shrink beneath you, and Larissa Noto’s phone buzzed somewhere around the tenth floor. It was her oncologist. He wanted her to come in the following week for a PET scan, a small thing, routine. She told him she could absolutely do that. She was feeling lucky. She was, after all, already in Vegas.
His whole voice changed. Vegas? What are you doing there? There are a lot of people there.
Two weeks earlier she had taken her last hard chemo infusion for HER2-positive breast cancer. Now she was about to drive to Zion to, in her words, hug a mountain.
The Instinct to Rest vs. The Science of Movement
His worry was real, and it was not about the hiking. Chemo knocks your immune system flat, and a casino in the middle of cold and flu season is a petri dish. Larissa knew that. She kept to her own suite, stayed outdoors, and went to hug a mountain instead of a blackjack table.
But underneath a doctor’s specific, reasonable caution sits a much older instinct, the one almost everyone aims at people in treatment without thinking: slow down, rest, let me carry that, don’t overdo it.
That instinct is the one that, more and more, the science says is wrong.
See Episode #7 with Dr. Jay Harness - Rest is Killing You - the science of Exercise Oncology
Larissa is a yoga and mindfulness teacher who spent years as a corporate attorney before she pivoted out of law for good. She talks about her body the way you talk about an instrument you have played for decades. When cancer arrived she was furious at it, and then she did the thing she teaches: she got underneath the anger, found the fear sitting under it, and got up and moved. By her own account she had been resting through the entire stretch of treatment. By the time the worst of the chemo was behind her, she was not looking for a sofa. She was looking for a trailhead.

Overcoming the Invisible Research
I should say up front that I am biased. A month before my own surgery, because I had to book the flights, I asked my plastic surgeon whether I could e-bike through vineyards in France. She looked at me and asked, “Will you use the e-bike part?” Yes. I had no interest in undoing fourteen hours of her beautiful work.
Six weeks after my bilateral mastectomy and reconstruction, I was “pedaling” through those vineyards. Three months out and cleared, I was wakeboarding. I lifted and did interval training the whole way through chemo. So when Larissa told me about Zion, I did not gasp. I recognized her.

Here is what neither of us could have explained at the time, even as we both did it on instinct, and what a surgeon named Dr. Jay Harness spent thirty-five years of operating without knowing. He told me on the show that he built some of the first integrated breast cancer centers in the country and performed mastectomies for three and a half decades before he stumbled onto exercise oncology, about eight years ago, when someone suggested he meet a woman named Andrea Leonard.
The science she described made his jaw drop. As he put it to me, “Why in the world did I not know about this?”
The answer was almost absurd. The research had been sitting in sports medicine and kinesiology journals since the 1990s, invisible to the oncologists treating the very patients it was about.
What the Guidelines Say Now
The old instruction was simple: rest, avoid activity, get on the sofa.
The National Cancer Institute now says plainly that early exercise research contradicted that advice (NCI Cancer Currents Blog) and that the field of exercise oncology now includes more than 1,000 randomized trials.
The American Cancer Society’s current guidance is close to the opposite of rest: survivors should build up to 150 to 300 minutes a week of moderate movement (ACS Nutrition and Physical Activity Guideline), plus strength work a couple of days a week, which eases the fatigue and treatment side effects most patients are told to simply endure.
Then last June the evidence stopped being suggestive and got loud.
The CHALLENGE trial, published in the New England Journal of Medicine, followed 889 colon cancer patients for nearly eight years (NEJM CHALLENGE Trial).
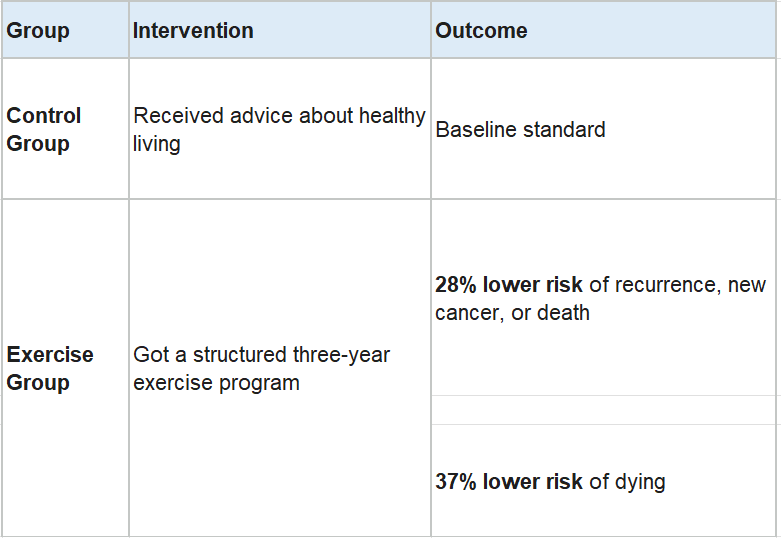
These results sit in the same neighborhood as chemotherapy. It earned a standing ovation at ASCO, and the journal ran an editorial telling oncology it was time to act (NEJM Editorial).
That trial was in colon cancer, so I will not pretend it proves the same numbers for Larissa’s breast cancer or my triple negative. The breast cancer evidence runs the same direction, though: physical activity after diagnosis is associated with a lower risk of dying from the disease (NCI Guidelines). Jay’s read was that my years of lifting had given me a real head start before I took a single drug. I’m sure Larissa’s yoga practice did the same for her.
Defiance with Discernment
Larissa did not ignore her oncologist. She heard the worry, mitigated the real part, and made her own informed call. I asked my surgeon before I touched that e-bike. The guidelines build in caution: get cleared, let surgical sites heal, protect an immune system that chemo has knocked down.
The point is not to overrule your care team. The point is to stop treating your body like glass, as research keeps insisting that movement may be part of what saves it.
Which brings me back to the elevator. Her oncologist heard Vegas and pictured crowds, germs, a body with its defenses down. Fair enough. So she stayed outside and pointed herself at a mountain, which is about the safest place a person with a flattened immune system can be, and which also happened to be doing her more good than a sofa ever would.
She hiked Zion the next morning. Then four more trails in Oregon, building her tolerance as she went, because that is how she does everything. Her oncologist wanted her safe. What she handed him was better than safe. She handed him a patient who was already doing the one thing the science keeps begging the rest of us to try.
I adored listening to your story, as well as sharing my own! Let's keep kicking cancer's A$$ together. A huge Thank You to you, @joellekaufman!
In 1990, I learned that I hade large cell lymphoma. A doctor told me "You will be cured or dead in 6 months. My treatment was harsh and involved high doses of radiation and aggressive chemotherapy. When I learned this news, I made two resolutions. I am not going to die until I am dead and I will live every day as normally as I can. During the chemotherapy, some of my days were not very normal, but I kept working as an internal medicine physician and attending my kids activities. I definitely hear both of these ladies.
It is no surprise that physical activity works. AMPK in our cell biology is a master genetic survival switch. Exercise activates that switch which in turn turns on many genes that promote our survival. This switch evolved to handle a crisis. If there is no food to support fetal growth, AMPK shuts down the growth pathways, and activates genes that pull calories from fat and muscle to support life in the vital organs until there is food again. It is a genetic survival switch for the fetus and it retains that function all throughout our lives. AMPK activation switches on the genes that are involved in cellular housekeeping (autophagy), mitochondrial health and replication, fighting inflammation and excess oxidants. Cancer mutations are caused by DNA strand breaks. AMPK repairs those breaks more accurately. AMPK activation promotes our survival in every way, including when we have cancer. I hope this helps Joelle's readers understank why getting off the couch is critical if you have cancer.