
The First Real Prevention Option for the Breast Cancers That Have Had None
The Long-Awaited Milestone in Personalized Preventative Care

My niece is eighteen. My daughter is nineteen. According to Dr. Sacha Howell, the mutations that eventually lead to breast cancer are, at this moment, beginning to appear in their bodies. Some of the women in my family carry BRCA1 — a mutation that runs through us like a thread. Even the women in my family who don’t carry it still carry the one-in-eight lifetime risk that comes with being a woman in the United States.
Here is what Dr. Sacha Howell told me at the Rise Up conference in San Francisco that I want every person with a daughter, niece, sister, wife, or female friend to know: the first genetic abnormalities that eventually lead to breast cancer appear in late adolescence. Not when the tumor shows up on a mammogram. Not in her thirties, when she finds the lump. In her teens. Quietly. Invisibly. Driven by the hormones that flood a young woman’s body every month from the time she gets her first period.
The cancer we diagnose at forty has, in a real sense, been twenty years in the making.
That changes what prevention has to mean. Prevention isn’t a middle-aged woman’s problem. It’s a life-course problem. And until very recently, the medicine for it has been stuck.
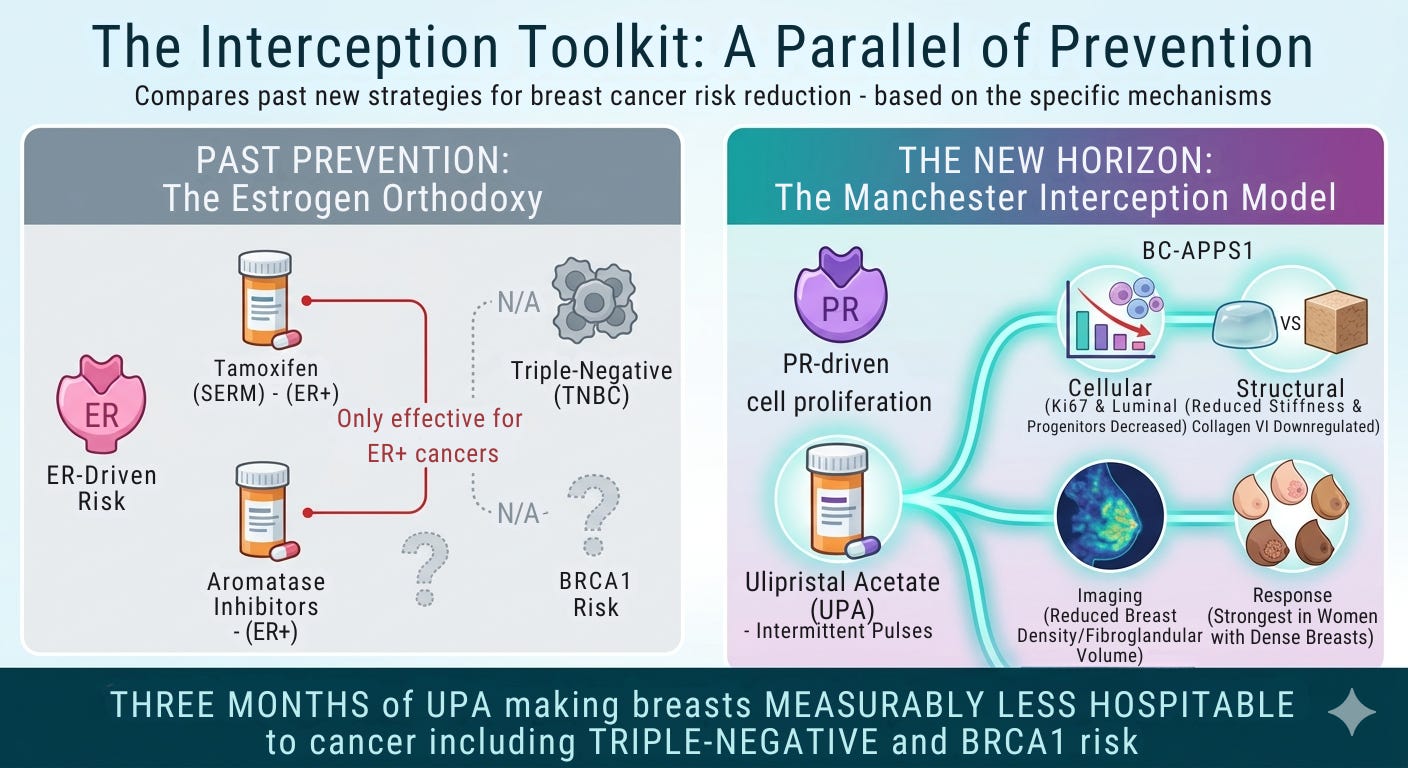
The estrogen orthodoxy — and the cancers it can’t touch
For four decades, breast cancer prevention has been organized around one hormone: estrogen.
Tamoxifen, a selective estrogen receptor modulator, was approved as a preventive agent in 1998.
Aromatase inhibitors, which block estrogen production itself, followed.
Both reduce estrogen’s effect on breast tissue. Both have been the only pharmacological prevention options available to high-risk women for an entire generation.
Here’s the catch: they only work on cancers that are driven by estrogen.
Triple-negative breast cancer (TNBC) isn’t. TNBC is the most aggressive subtype, the one most likely to recur in the first few years after diagnosis, and the one BRCA1 carriers are statistically most likely to develop at a younger age. For TNBC risk, tamoxifen does nothing. Aromatase inhibitors do nothing. The only options have been surgical — prophylactic mastectomy and oophorectomy — or active surveillance with no pharmacological intervention to actually lower the underlying risk.
Two-thirds of women who develop breast cancer have no family history. The Wisdom Study has shown that polygenic risk scoring can identify many of those women before cancer appears, opening the door to anti-estrogen prevention for those whose risk is hormone-receptor-driven. That’s real progress — and it’s still incomplete. For the women at risk is for triple-negative disease, no prevention drug has existed. Until now.
The Manchester Breast Centre’s discovery
Between 2016 and 2019, Dr. Howell’s team at the Manchester Breast Centre ran the Breast Cancer Anti-Progestin Prevention Study — BC-APPS1. Twenty-four premenopausal women with a strong family history of breast cancer took ulipristal acetate (UPA), 10 mg daily, for twelve weeks.
The results, published in Nature in November 2025 (Simões et al., DOI: 10.1038/s41586-025-09684-7), are the most rigorous evidence to date that anti-progestins can modify the precursor biology of breast cancer:
Cellular: Ki67 staining (a standard proliferation marker) dropped significantly. Luminal progenitor cells — the putative cells of origin for triple-negative breast cancer — decreased in proportion, proliferation, and colony-forming capacity.
Structural: Atomic force microscopy showed that the breast tissue became less stiff. Collagen VI, a key extracellular matrix protein associated with tumor-supportive architecture, was dramatically downregulated.
Imaging: MRI showed reduced fibroglandular volume, which maps onto reduced breast density, one of the most consistent independent risk factors for breast cancer.
Response profile: Women with dense breasts at baseline responded most strongly.
In plain English: three months of a drug already on U.S. pharmacy shelves made these women’s breasts measurably less hospitable to cancer — including the kind of cancer no other prevention drug has ever been shown to touch.
Why is this not front page news?
Ulipristal acetate has been prescribed to roughly one million women in Europe for uterine fibroid treatment. Five of those women developed liver failure — a serious outcome, but at a rate of one in 200,000.
The European Medicines Agency suspended the drug. That decision wasn’t unanimous. The agency’s own published assessment documents the internal disagreement: one committee wanted a full ban, another pushed back, and the drug was eventually reinstated for limited fibroid use in Europe. In the U.S., ulipristal acetate remains FDA-approved as Ella, prescribed regularly by OB/GYNs as emergency contraception.
Now compare that one-in-200,000 rate to drugs regulators have not pulled:
Statins (prescribed to roughly 40 million Americans) carry documented risks of liver injury and, rarely, rhabdomyolysis.
Combined hormonal contraceptives carry blood-clot risks well above the 1-in-200,000 threshold.
Baseline breast cancer mortality: In the UK, roughly 30 in 200,000 women in their forties die from breast cancer each year. Thirty times the UPA liver-injury rate.
A narrative review co-authored by Dr. Liberty and colleagues in Contraception in 2025 (Ebersole et al., PMID: 40044021) reached a blunt conclusion: the liver-injury signal was never confirmed, preclinical studies hadn’t predicted it, and access to UPA matters for conditions ranging from emergency contraception to fibroids to — now — breast cancer prevention.
What Dr. Howell hypothesizes next
He believes the path forward isn’t continuous lifelong use. It’s pulses — three-month courses of UPA, spaced across a woman’s reproductive life. Fifteen to twenty years of intermittent treatment could meaningfully reduce the cumulative number of luteal phases a woman experiences.
Fewer cycles means fewer cellular divisions, which means fewer chances for the mutations that begin in adolescence and accumulate, silently, until the day the mammogram catches what’s been growing for decades.
It’s a genuinely new model of prevention — one that treats breast cancer risk the way cardiologists treat cardiovascular risk: long-term, calibrated pharmacological management based on individual risk stratification.
What you can do
If you’re high-risk (BRCA-positive, strong family history, or a polygenic risk score above threshold), bring the Nature paper to your OB/GYN. High-risk women without cancer don’t have oncologists. The conversation has to start in your gynecologist’s office.
If you’re in the U.S. and 30 or older with no personal history of breast cancer, enroll in the Wisdom Study. Risk-stratified screening is the infrastructure that prevention drugs need.
If you have a daughter, a niece, a wife, a friend, or a younger sister, this matters now. Not when she finds a lump. Now.
The mutations start in adolescence. The science is finally beginning to catch up to the biology — and the regulatory framework around it has to catch up too.
The science isn’t waiting. The regulators are.
This episode of Kicking Cancer’s Ass is sponsored by Paxman Scalp Cooling. Full episode with Dr. Sacha Howell: [Spotify] | [Apple Podcasts] | [YouTube].