
The Cancer Advice Is Right. That’s Exactly Why It Stopped Working.
We turned real prevention into background noise.

We’re natural optimists, all sure the cancer happens to someone else, so the WHO’s cancer prevention advice, reiterated this week in a call for “urgent action” against a new projection that cases will nearly double by 2050, doesn’t result in individual change without a long-term government effort (see South Korea!). Knowing your inherited risk is what makes the odds personal, if we make it accessible, affordable, and safe to know.
The mammogram is due. You know it means a half day you can’t spare, a drive across town, a paper gown, and two days waiting for a call you’re afraid to answer. So it slides to next month, then next year. And that’s the easy version, the one where a machine exists within reach at all. For millions of women, the nearest one is hours away, booked months in advance, or not there. Screening is the tool we lean on hardest, and the one we’ve made hardest to use.
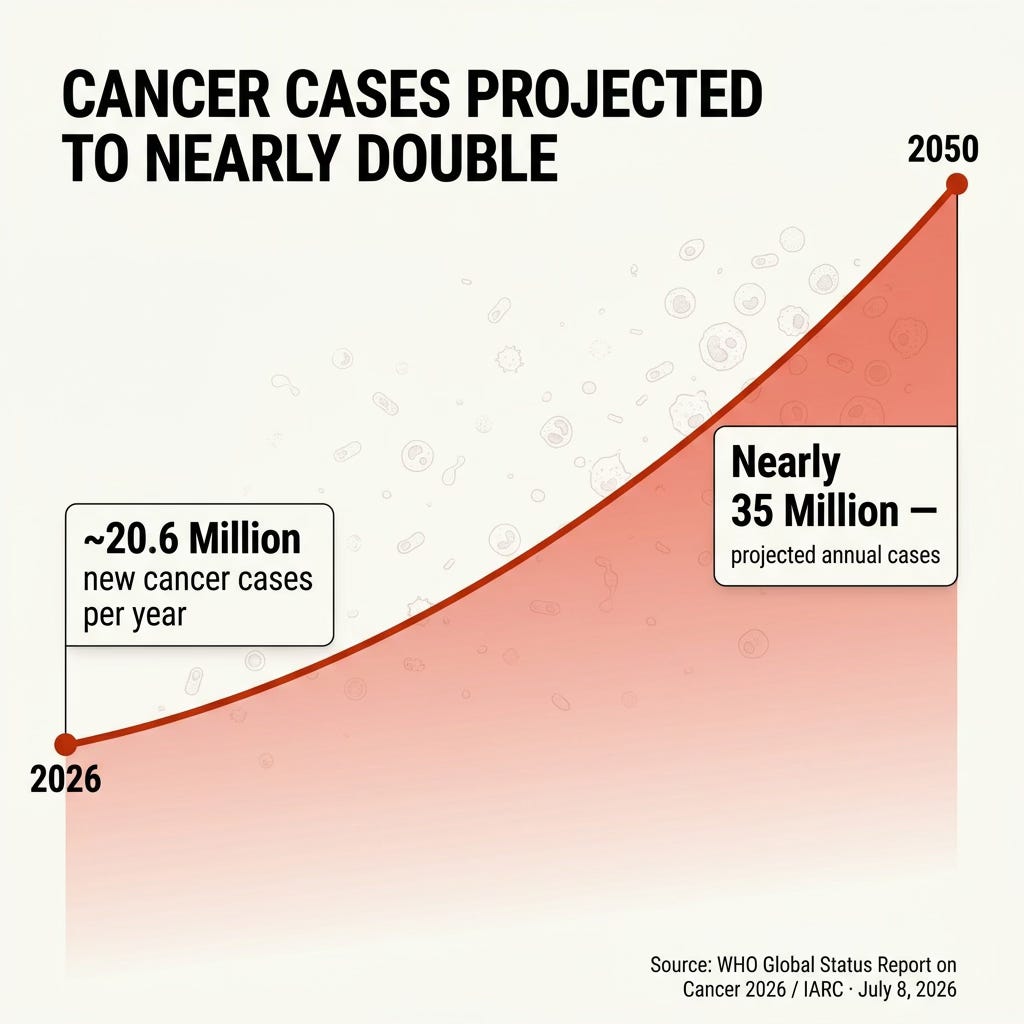
This week the World Health Organization put a number on that. New cancer cases, around 20 million a year now, are projected to reach nearly 35 million by 2050, and cancer is already the second leading cause of death in the world. The new WHO Global Status Report on Cancer 2026, built with the International Agency for Research on Cancer, lays out a wave we can still get ahead of, if we use the right tools.
Most of the report’s prevention advice is correct, and you already know every word of it. Don’t smoke. Eat real food. Move your body. Nearly four in ten cancers can be traced back to risks like these. All true, and repeated for decades: warning people off cigarettes for sixty years, nagging them about food and exercise for forty, in so many pamphlets and campaigns that it stopped sounding like information and started sounding like weather. Correct advice nobody hears isn’t a strategy. It’s background noise. The science isn’t the problem. The marketing is.
Leslie Zane has spent thirty years proving this from the other side. Her brand consultancy, Triggers, and her book, The Power of Instinct, rest on one finding: the unconscious mind, not the reasoning one, decides what we trust, buy, and ignore. Winning brands don’t argue with you; they plant themselves in your instinct until choosing them feels automatic. I spoke with her last week, and my mind heard a novel approach to cancer control in everything she said about brands. Prevention runs the opposite play. It feeds the conscious mind statistics, and the conscious mind is barely driving. A cancer number is abstract; it belongs to a population, and the optimist in the back of your skull has already filed it under happens to someone else. It isn’t losing to bad science. It’s losing to a brain that saves its shelf space for what feels like it’s coming for you. The fix isn’t more facts. It’s the discipline Zane sells to the Fortune 100, aimed at the one product nobody markets: your own survival.
Buried in that same bucket are two novel and important things. The HPV vaccine stops the infection behind nearly all cervical cancer and much throat, anal, and other cancer. Not a lifestyle or a habit you white-knuckle for decades. A pair of shots cover you for life. And Helicobacter pylori, a common stomach bacterium, can be caught with a breath test and cleared with antibiotics, cutting the risk of stomach cancer, one of the deadliest in the world. Neither has anything to do with your genes; these prevention interventions work for everyone. Their problem isn’t that people don’t feel at risk. It’s that too few consumers know they prevent cancer at all. That’s the headline, and we keep printing it as fine print.
Genetics is the one thing that beats the optimism. “You could be at risk” is easy to shrug off. “You are at risk, and here is your number” is not.
A small group inherits a single high-impact mutation, for example, the BRCA1, BRCA2, and Lynch syndrome variants that carry heavy risk on their own, the 5 to 10 percent we’ve long called hereditary. The WISDOM study, whose first results were released late last year, found that 30 percent of women carrying one of those BRCA1 or BRCA2 mutations had no family history at all. The old rules, which test only people with a family history, would have missed every one of them.
The WISDOM study, whose first results were released late last year, found that 30 percent of women carrying one of those BRCA1 or BRCA2 mutations had
no family history at all.
The rest of us carry a quieter kind of risk: hundreds or thousands of tiny, common variants that mean little alone and a great deal together. A polygenic risk score reads that whole pattern and puts a real number on your susceptibility. WISDOM used those scores to move 12 to 14 percent of women into a different risk category than their age would have assigned. Some higher, some lower.
Two honest caveats, before anyone else raises them. WISDOM is a trial, not yet a guideline, so this is a direction rather than a settled protocol. And today’s risk scores were built mostly on European genomes, so they perform poorly on other ancestries. That is not a reason to wait. It is a reason to build on the science everywhere, which is already happening. At June’s ISOPT Congress, Dr. Ning Liao of Guangdong Province People’s Hospital showed that the inherited-risk map in Chinese breast cancer patients isn’t the Western one: their most common BRCA mutation is BRCA2, not BRCA1, and their tumor genetics diverge from the textbooks written on Western patients. Port a European tool onto them and you get the wrong answer. The fix is population-specific genomics, built group by group.
The fix is population-specific genomics, built group by group.
My mother was 36 when she was diagnosed. My sister was 29. Both are survivors. Both were more than a decade under the age the guidelines say screening should even begin. Their risk was real and early, and no calendar was ever going to catch it. A number would have.
A personal number turns a statistic into a reason to act, and the proof is in the people who already know theirs. In one international study, 64 percent of women who learned they carried a BRCA mutation chose risk-reducing surgery, most within the year, and close to 70 percent of Lynch syndrome carriers did the same within three years. A number gets people to the screening they would otherwise skip, and it fixes the burden we started with: send the intensive screening to the people whose biology says they need it, and spare the ones it was only ever going to frighten. Screen by risk, not by age alone.
Screening is one thing. Daily habits are another matter, and here the number alone is not enough. The same result that gets people screened doesn’t change what they eat or whether they move. The best trials handed people their genetic risk and found no change in diet or activity months later. That isn’t a character flaw. It’s how behavior works.
Wendy Wood has spent three decades on this. Roughly 43 percent of what we do in a day is on autopilot, driven by context rather than intention, which means the scary statistic and the New Year’s resolve push on the wrong lever. Willpower is not the mechanism. Design is. You change a behavior by changing the cues and the friction around it, not by wanting it more.
Willpower is not the mechanism. Design is. You change a behavior by changing the cues and the friction around it, not by wanting it more.
- Wendy Wood
So the move isn’t to try harder. It’s to build the behavior into your life so it runs without a daily vote. Here are two examples from my life:
I work out three times a week at 6:30 with my closest friend, same days, in person or on video. It isn’t a fitness plan; it’s our standing date, the way we actually talk. The workout rides along on something I already want, time with her, and neither of us bails when the other is waiting. Behavioral scientists call the pieces of that implementation intentions and temptation bundling. I call it the only reason I’m up at 6:30.
My husband and I turned Sunday into the farmer’s market and a couple of hours of prep together. A date, not a chore. By Sunday night, the good food is washed, cut, cooked, and at eye level in the fridge, so all week the healthy choice is the easy one and the junk takes effort. That’s Wood’s whole point: stop leaning on willpower and rearrange the friction.
Stop leaning on willpower and rearrange the friction.
- Wendy Wood
None of that needs a genetic test. The test is what makes you commit; the habits are what make it stick.
So treat genetic risk as what it is: a public health catalyst, the thing that turns decades of ignored advice into action people actually take. To work at the scale the WHO is projecting, it has to be three things.
Accessible,
So a risk score isn’t a perk for people who already have good doctors, and never one more thing the wealthiest systems have, and the rest don’t. The report’s own numbers show the stakes: five years after a breast cancer diagnosis, 87 percent of women in high-income countries are alive, against 42 percent in the lowest-income ones. Same disease, opposite odds, mostly a matter of access. A prevention tool that reaches only the countries already winning would widen that gap. The whole point is to close it.Affordable,
So knowing your risk never depends on the size of your paycheck.And risk-free.
The biggest reason people refuse a genetic test, if one is even available in their region, isn’t fear of the result. It’s fear of what the result will cost them everywhere else. In the United States, GINA, the Genetic Information Nondiscrimination Act of 2008, barred health insurers and employers from using your genetics against you. Good, as far as it goes, which isn’t far: life, disability, and long-term care insurers are still free, under federal law, to ask, to know, to charge more, and to turn you away. And GINA is only a US law; most of the world has nothing like it. Even nationalized healthcare only takes insurance pricing off the table. It does nothing about an employer who treats your result as a liability, or a community that looks at you differently once your DNA is on the record. Ask people to learn their risk while those doors stand open, and plenty decide they’re safer not knowing. The catalyst never fires.
Cancer cases doubling by 2050 is a projection, not a verdict. We already have a vaccine, a bacterial test, and the power to hand people their own risk as a number they can’t ignore. What we’re missing is the will to make all of it easy to reach, easy to afford, and safe to know.
You don’t pick the pitch. You control your swing. But first you have to see it coming.